Annex A: Key SBCC Theories in FP
When designing an SBCC program, one or a combination of theories can be used to guide both messages and approaches.
For example, using the Diffusion of Innovation (DOI) theory in a rural FP program where most women 35 years or older have not been to school and have little access to mass media highlights the powerful role change agents can play in changing behaviors in such communities.
If the change agents are “positive deviants ” who have successfully adopted birth spacing, they can be excellent messengers of FP method safety and showcase how a smaller family size allows them to make money and help support their families. As these messages spread throughout and between communities, more and more women may adopt modern FP methods.
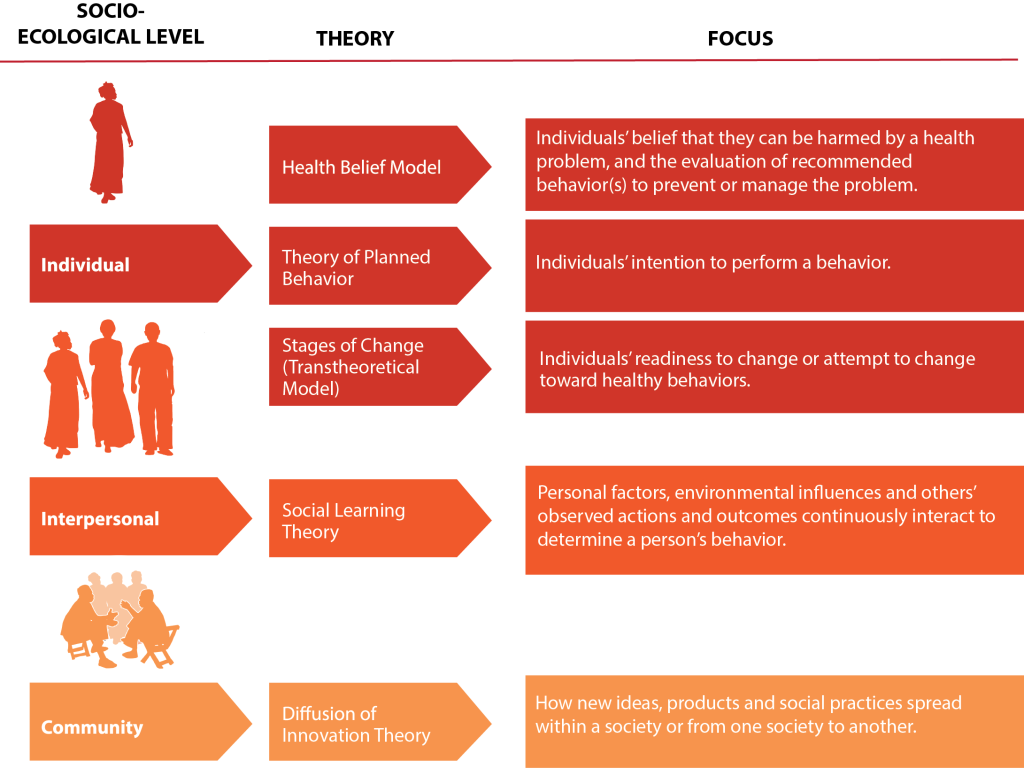
The Figure below displays the most commonly used behavior change theories in SBCC programs and identifies the intervention level according to the socio-ecological approach described in Section 3: Use SBCC to Address AMA and HP Pregnancies. Also in this annex are detailed explanations of each theory, and examples of how each theory can be applied in SBCC programs .

Resources
Not sure what theory to use?
Try TheoryPicker, an interactive tool that helps you identify what might be the best behavior change theory for a given program. The tool takes you through a number of steps and you answer a number of different questions to help determine which is the best theory or group of theories to use for your program design.
Key SBCC Theories
- Health Belief Model
- Theory of Planned Behavior
- Stages of Change
- Social Learning Theory
- Diffusion of Innovation
Health Belief Model

What Does the Health Belief Model Tell Us about Behavior?
The Health Belief Model highlights how programs need to consider individual beliefs about the problem being addressed and the costs and barriers associated with changing a behavior. The Health Belief Model is based on the understanding that a person is likely to change behavior if he/ she experiences:
Perceived susceptibility/seriousness: one believes he/she is at risk. For example, a woman believes she is at risk of AMA or HP pregnancy-associated health risks.
Perceived benefits: one believes that the behavior change will reduce risk. For example, a woman believes that using contraception will prevent her from having an AMA or HP pregnancy.
Perceived barriers: how one interprets the cost/barriers of the desired behavior. For example, a woman believes that her partner would not want her to use contraception, but, for her, the benefits of using contraception to prevent a high-risk pregnancy outweigh his reaction.
Cues to action: strategies to activate “readiness.” For example, a woman receives education about contraception and the different options available to her.
Self-efficacy: confidence in one’s ability to take action. For example, a woman feels confident that she can access contraception and that she can use it correctly to avoid unintended pregnancy.
How Can the Health Belief Model Be Applied?
The Health Belief Model is best used when promoting individual preventive behaviors, such as condom use or getting vaccinations. It focuses on the beliefs and perceptions of the individual, so it is appropriate to change behaviors that are not heavily influenced by society and social norms. It tells us the importance of highlighting both the negative consequences of the current behavior and the positive consequences of alternative, suggested behavior.
For example, women in some cities in Sub-Saharan Africa are delaying starting a family until later in life to finish school and start a career. However, not all women are aware of the risks having a pregnancy later in life might bring. Program managers can use the Health Belief Model to help plan targeted programs for young women wishing to delay pregnancy that inform them about AMA pregnancy dangers and help them plan to start a family at an age and time that is right for them in their life, and to space pregnancies to make sure they safely have the number of children they want.
Theory of Planned Behavior
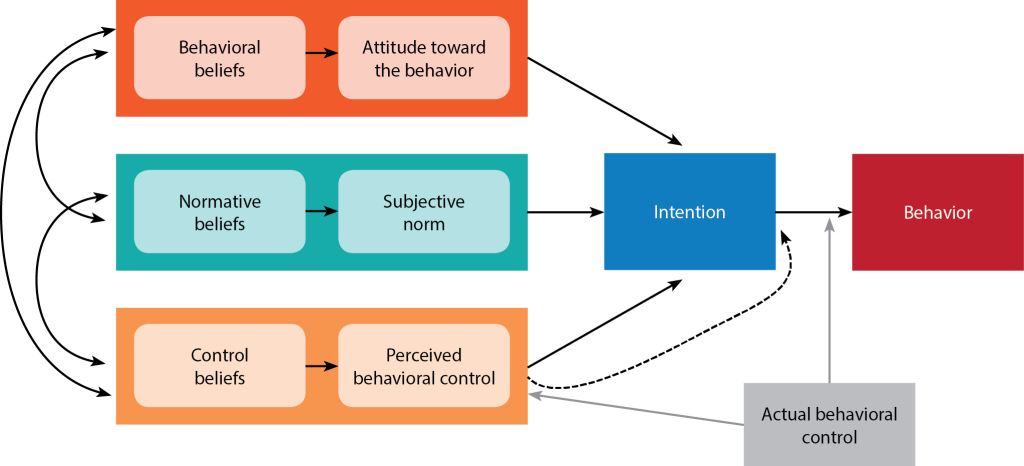
What Does the Theory of Planned Behavior Tell Us about Behavior?
According to the Theory of Planned Behavior (the original insight of Theory of Reasoned Action), behavior is influenced by three elements:
Attitude: that the behavior will be beneficial to the individual. For example, a woman feels that using a modern FP method is a good way for her to practice birth spacing.
Subjective norms: the belief that other people think that the behavior is acceptable. For example, a woman believes her partner, friends and family would support her using a modern FP method.
Perceived ability: the belief that one has the skills and capability to change behavior. For example, a woman believes she is able to access and use a modern FP method successfully for HTSP.
How Can the Theory of Planned Behavior Be Applied?
The Theory of Planned Behavior can be used to change behaviors that are heavily influenced by peers and the close social network. This theory tells us that the close social network needs to be targeted to support the desired behavior change in the individual, as well as that it is important to highlight the short-term benefits of the behavior change to promote action.
In Lomé, Togo, for example, there are several quality FP services and many women know and use modern FP methods and understand the opportunities using a method might offer them. However, there are rumors about the dangers of modern methods, such as infertility, and non-users question whether they should trust these “scientific,” artificial methods. The Theory of Planned Behavior helps programmers plan interventions that reach non-users with accurate FP method information. These messages are delivered by the most credible experts and role models to help dispel rumors and build confidence in modern FP methods.
Stages of Change

What Does Stages of Change Tell Us about Behavior?
The Stages of Change theory (sometimes called the Transtheoretical Model) tells us that individuals go through different stages when changing a behavior. This theory assumes that individuals have different degrees of motivation and readiness to change, which determine their current stage of change. According to this theory, different stages of change require different information needs and approaches to try and move the audience to the following stage. Although people may move through these stages in a predictable way, an individual can drop back or jump over stages. The stages are:
Precontemplation: There is no intention to change behavior in the future. For example, a woman is not thinking about using contraception to avoid an AMA or HP pregnancy.
Contemplation: An individual is aware that the problem exists and is seriously thinking about overcoming it, but has not yet made a commitment to take action. For example, a woman has learned about modern FP methods and is thinking about starting to use one.
Preparation: An individual intends to take action immediately. For example, a woman is planning to go to the health facility this month to start using a modern FP method.
Action: An individual begins performing the behavior. For example, a woman starts using a modern FP method to space her pregnancies.
Maintenance: An individual continues the behavior and works to maintain it. For example, a woman continues using the modern FP method of her choice consistently and correctly.
Some SBCC professionals have added a sixth stage to this model – Advocacy. Advocacy is the stage in which a woman is maintaining her use of a modern FP method, as well as promoting the benefits of modern FP methods to her friends and encouraging them to try it, too.
How Can Stages of Change Be Applied?
Stages of Change can be used in one-to-one situations, for example, between a client and a counselor. Knowing the stage of change of the client can help the counselor select what information to share. Information at the precontemplation and contemplation stages would focus on facts, the risks of the current behavior and the benefits of changing behavior. At the preparation and action phases, it would focus more on opportunities for changing behavior and how to access them.
In some countries pregnancy itself is seen as a high-risk situation in general, and AMA and HP are not seen as particular risk contributors. The Stages of Change theory can help program managers plan interventions to help men and women better understand the dangers of AMA and HP pregnancies and help prepare them for action to prevent these high-risk pregnancies from occurring in their household and family.
Social Learning Theory
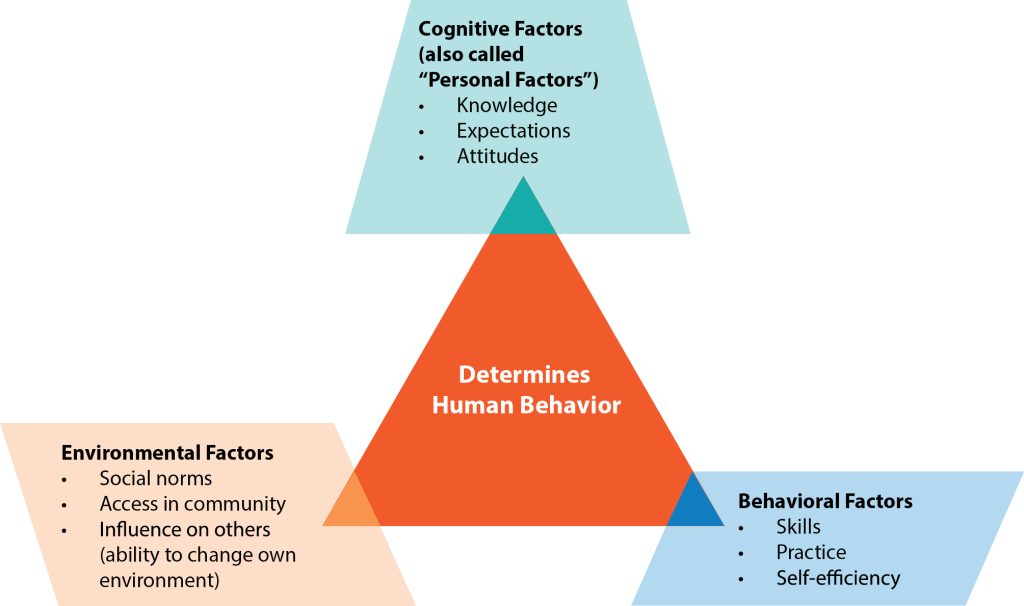
What Does Social Learning Theory Tell Us about Behavior?
Social Learning Theory acknowledges the interaction that occurs between an individual and his/her environment. The outside environment is where a person can observe an action, understand its consequences and become motivated to repeat it and adopt it. Behavior is affected by structural factors such as service availability and policies, as well as by social factors such as social norms and peer influence.
In the application of the Social Learning Theory, the learner (audience) is encouraged to:
Observe and imitate the behavior of others. For example, a woman may observe her friend using modern FP methods and therefore decide that she wants to use a modern FP method too.
See positive behaviors modeled and practiced. For example, a woman sees that her friend is happy with the modern FP method she has chosen. This makes her want to copy and model the same behavior.
Increase his/her own capability and confidence to implement new skills. For example, when a woman’s community becomes more supportive of and vocal about access to modern FP methods for AMA or HP women, she gains the confidence to talk to her partner about using a modern FP method.
Gain positive attitudes about implementing those skills. For example, after learning about how to use a modern FP method, a woman feels confident that she can maintain use and keep on track to spacing her pregnancies.
Experience support from his/her environment to use those skills. For example, a woman sees that the happy families on her favorite soap opera have fewer than five children and that encourages her to think that she can be happy with three to four children.
How Can Social Learning Theory Be Applied?
Social Learning theory can be used for behaviors that are heavily influenced by both the physical and social environment in which the individual lives. The theory tells us the importance of creating an enabling environment, in which the desired behavior change is made easier. It also tells us that seeing the behavior in practice can help others adopt it. This can be done through modeling, where the desired behavior, as well as the resulting benefits, can be demonstrated and popularized by role models.
Limiting births to fewer than five per family may seem unthinkable in some countries, for example. However, if the government has projected the costs of a large population on infrastructure, education, health, agriculture and security, they may be convinced that reducing family size is in the interest of the nation, as well as the household. Modeling lower family sizes may be done through reality TV and other mass media or through testimonials from political and community leaders, as well as those women who have chosen a smaller family size.
Diffusion of Innovation
What Does Diffusion of Innovation Tell Us about Behavior?
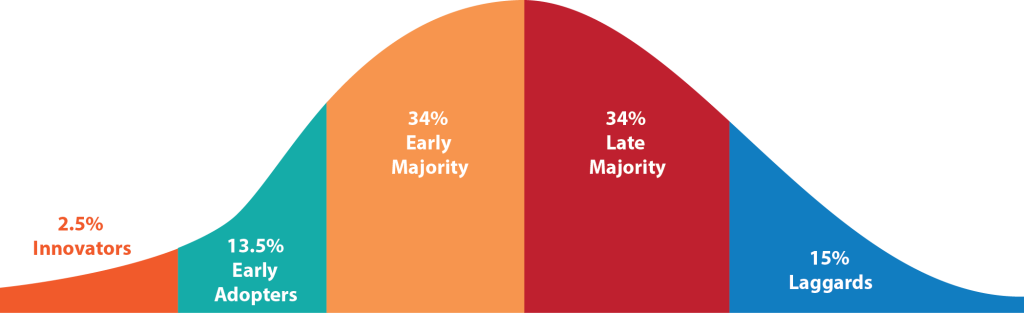
Diffusion of Innovation refers to the spread of new ideas and behaviors within a community or from one community to another. Some individuals and groups in society are quicker to pick up new ideas, or “innovations,” than others. This theory identifies five categories that define a person’s propensity to accept or adopt the innovation:
- Innovators: the quickest to adopt an innovation. However, they may be seen as fickle by other community members and are less likely to be trusted and copied.
- Early adopters: more mainstream within the community and are characterized by acceptance of innovation and some personal/financial resources to be able to adopt the innovation.
- Early majority: amenable to change and persuaded of the benefits of the innovation by observing.
- Late majority: skeptical and reluctant to adopt new ideas until the benefits are clearly established.
- Laggards: these are most conservative and resistant to change; sometimes, they may never change.
The likelihood of adopting an innovation/behavior depends on the audience, environmental barriers and facilitators, the communication system and the innovation’s attributes, such as:
Relative advantage: does the behavior offer an advantage over the current behavior? For example, does using a modern FP method offer a woman a benefit (e.g. better health) she currently doesn’t have?
Compatibility: is the behavior compatible with prevailing social and cultural values? For example, is it culturally acceptable for a woman with five children to use a modern FP method?
Complexity: how difficult is the new behavior to perform? For example, would a woman be able to manage using a modern FP method (i.e., taking a pill everyday, getting a shot on schedule)?
Triability: can the behavior be tried out without too much risk? For example, is it possible for a woman to try out a modern FP method and see what it’s like?41
Observability: are there opportunities to see what happens to others who adopt the behavior? For example, does a woman have friends who are using modern FP methods that can talk to her about it?
How Can Diffusion of Innovation Be Applied?
Diffusion of Innovation can be used to change behaviors that are influenced by social norms and social trends. The theory tells us how to promote the desired behavior by focusing on attributes. This can be done through agents of change, that is, the early adopters of a new behavior who promote it and encourage others to adopt it. Agents of change can be people working in the community or community members who have adopted the new behavior and can act as role models. Targeting effective agents of change, such as local leaders, influential individuals, peers and celebrities can accelerate the adoption of a new behavior.
For example, in countries where rural women 35 years or older have not been to school and have little access to mass media, change agents can be very powerful to bring new technologies or behaviors to rural communities. If the change agents are “positive deviants” who have successfully adopted FP, they can be excellent messengers of the safety of using FP, showcasing how a smaller family size can allow them to make money and help support their families. As these message spread throughout and between communities, more and more women may adopt modern FP.
- Annex A: Key SBCC Theories in FP
- Annex B: Illustrative Positioning Statements
- Annex C: Communication Approaches and Activities
- Annex D: Client Brochure for Less Conservative Audiences
- Annex E: Client Brochure for More Conservative Audiences
- Annex F: Guide for Working with Community-Based Groups
- Annex G: Counseling Guide for Providers
- Annex H: Counseling Guide for CHWs
- Annex I: Provider Reminder Poster
- Annex J: Guide for Researchers
- Annex K: Guide for Journalists
- Annex L: Infographics for Health Priority Decision-Makers