Social and behavior change communication (SBCC) uses communication to change behaviors by positively influencing knowledge, attitudes and social norms. Research shows that SBCC works and has been effective in a variety of health areas, such as HIV and family planning. Here we show its impact on emerging pathogens - in particular Ebola.



Whether it is SARS, H1N1, Ebola or, now, the Zika virus, emerging pathogens continue to challenge public health experts. Because of the emergent nature of the pathogen, effectively responding to these outbreaks in real time always requires the use of social and behavior change communication (SBCC) while other solutions (vaccines, treatments, etc.) are sought.
This was the case with Ebola, which spread to Liberia in spring 2014 from Guinea and then within West Africa. When all was said and done more than 11,000 died, but SBCC played a crucial role in stemming the spread by calming fears, dispelling rumors, providing answers and pulling together a coordinated response.

Ebola flared up in Lofa County, Liberia, near the Guinean border in March 2014, but the situation appeared to stabilize throughout April and May. Then in June, Liberia reported 51 cases and the virus quickly spread to the capital city of Monrovia, where it rapidly overwhelmed the health care system. By September 2014, Liberia reported nearly two thousand cases and more than one thousand deaths.


Source: WHO

Dec 2013
Jan 2014
Feb 2014
Mar 2014
Apr 2014
May 2014
Jun 2014
Jul 2014
Aug 2014
Sep 2014
Oct 2014
Nov 2014
Dec 2014
Jan 2015
Feb 2015
Mar 2015
Apr 2015
May 2015
Jun 2015
Jul 2015
December 6, 2013
Patient Zero
March 31, 2014
First Case Reported in Liberia
June 17, 2014
Ebola Hits Monrovia
July 30, 2014
Liberia Shuts Down its Schools
August 4, 2014
Liberian Government Mandates Cremation for Ebola Victims (increasing secret burials)
August 8, 2014
Liberia Call Center Launched
September 16, 2014
US to Send Troops to West Africa
November 2, 2014
Rapid Community Assessments on Safe Burial
May 9, 2015
Liberia Declared Ebola Free
June 30, 2015
Ebola Returns to Liberia

Medical interventions were not stemming the outbreak and throughout June, July and August of 2014, more and more people were dying and very few were surviving. The Liberian Ministry of Health (MOH) along with international and national NGOs quickly realized prevention messaging and community/social mobilization efforts were needed to reach communities to underscore the need to change behaviors related to long-standing cultural practices. Communities needed timely and credible information, but it was also critical that they felt ownership of their response to the crisis. Early messaging such as “Ebola Kills” created fear and confusion. The MOH had to convince communities that Ebola was deadly, but you could survive if you sought help early.


Gathering research in such a chaotic time and place was clearly a challenge. Doubts about methods of transmission and prevention strategies further created confusion, fear and mistrust among those in the affected areas. At the time, data was not available about the public’s level of knowledge of the Ebola virus, its modes of transmission and what kind of information communities needed to guide their response and help curb the epidemic.
Surveys were conducted via text messaging using mobile phones to quickly gather on-the-ground perceptions and knowledge of the virus among affected communities. This high-tech, low-touch method kept door-to-door surveyors away from potential exposure to the virus.
In November 2014, the USAID-funded Health Communication Capacity Collaborative (HC3) partnered with an SMS-based survey company called GeoPoll to design and disseminate a questionnaire that would produce a rapid assessment.

Source: DHS and WHO
Within three days of the survey launch, 1,000 men and women over the age of 15 completed the questionnaire by replying to texts from GeoPoll. These results along with other demographic information and survey data gathered through more traditional methods helped SBCC professionals develop a communication response and strategy with little wait time. (Just what a fast-moving epidemic called for.)


Above are selected questions taken from the Rapid Assessment GeoPoll survey; scroll through a sample of the results from the same survey.

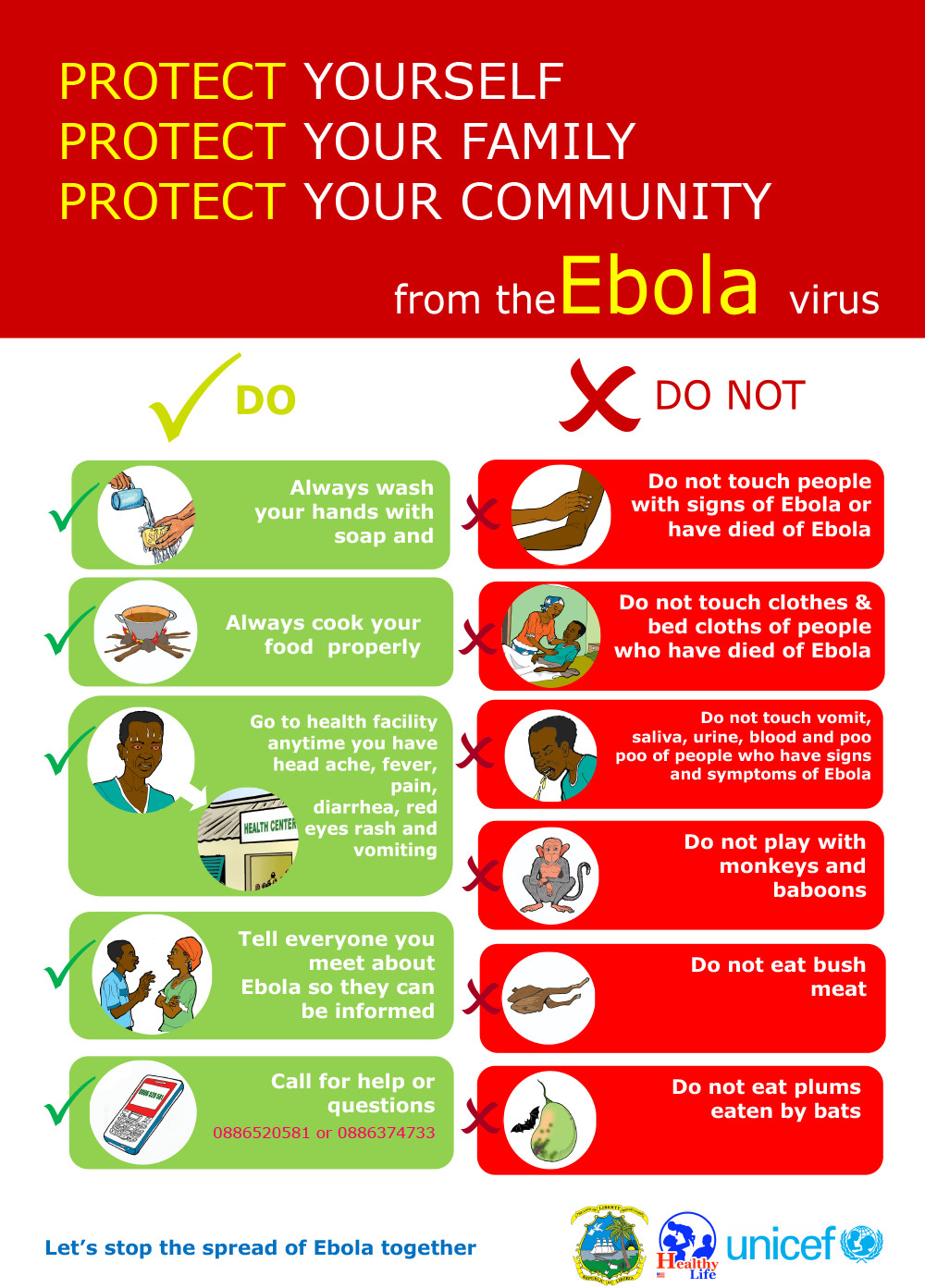
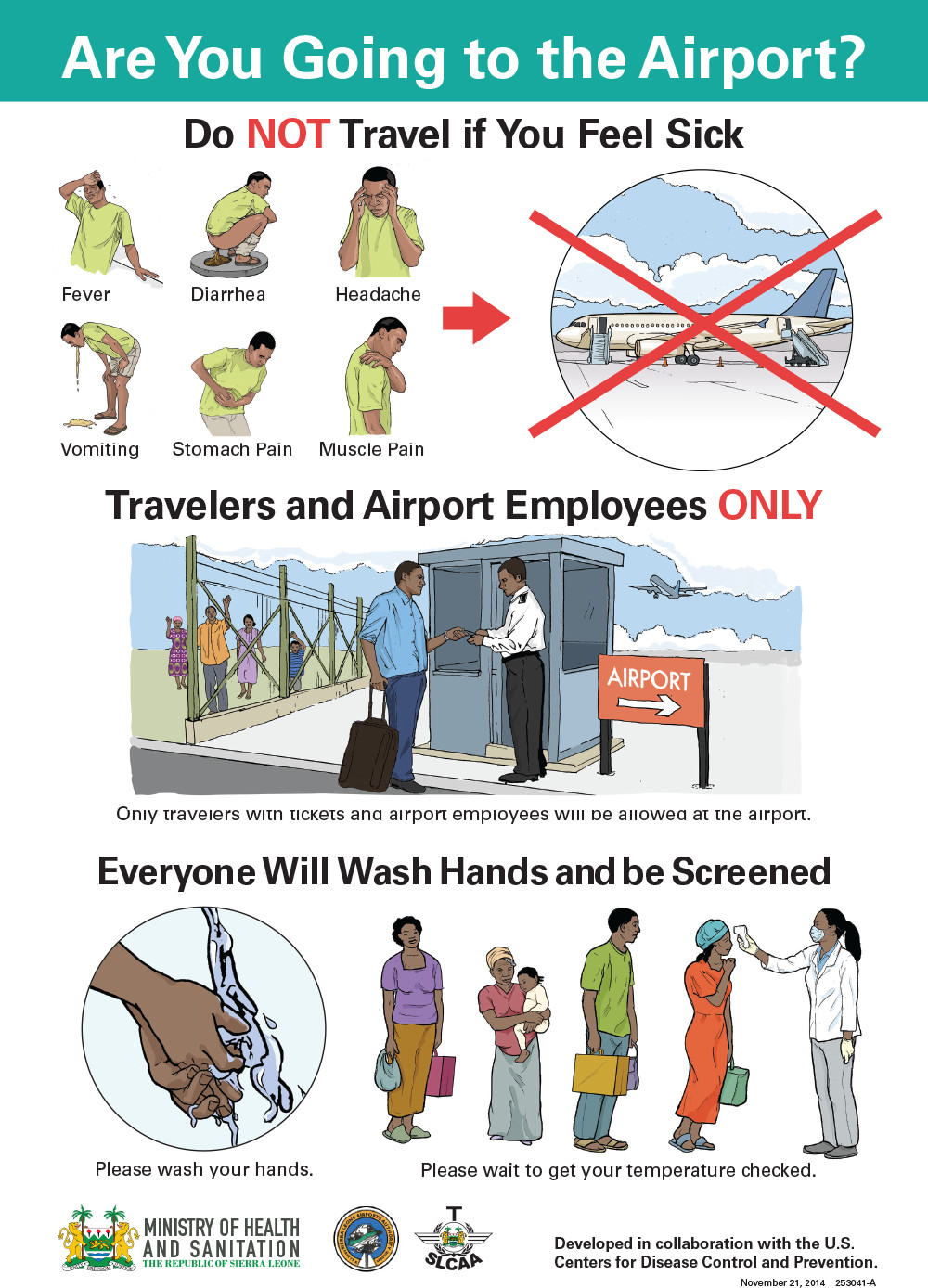
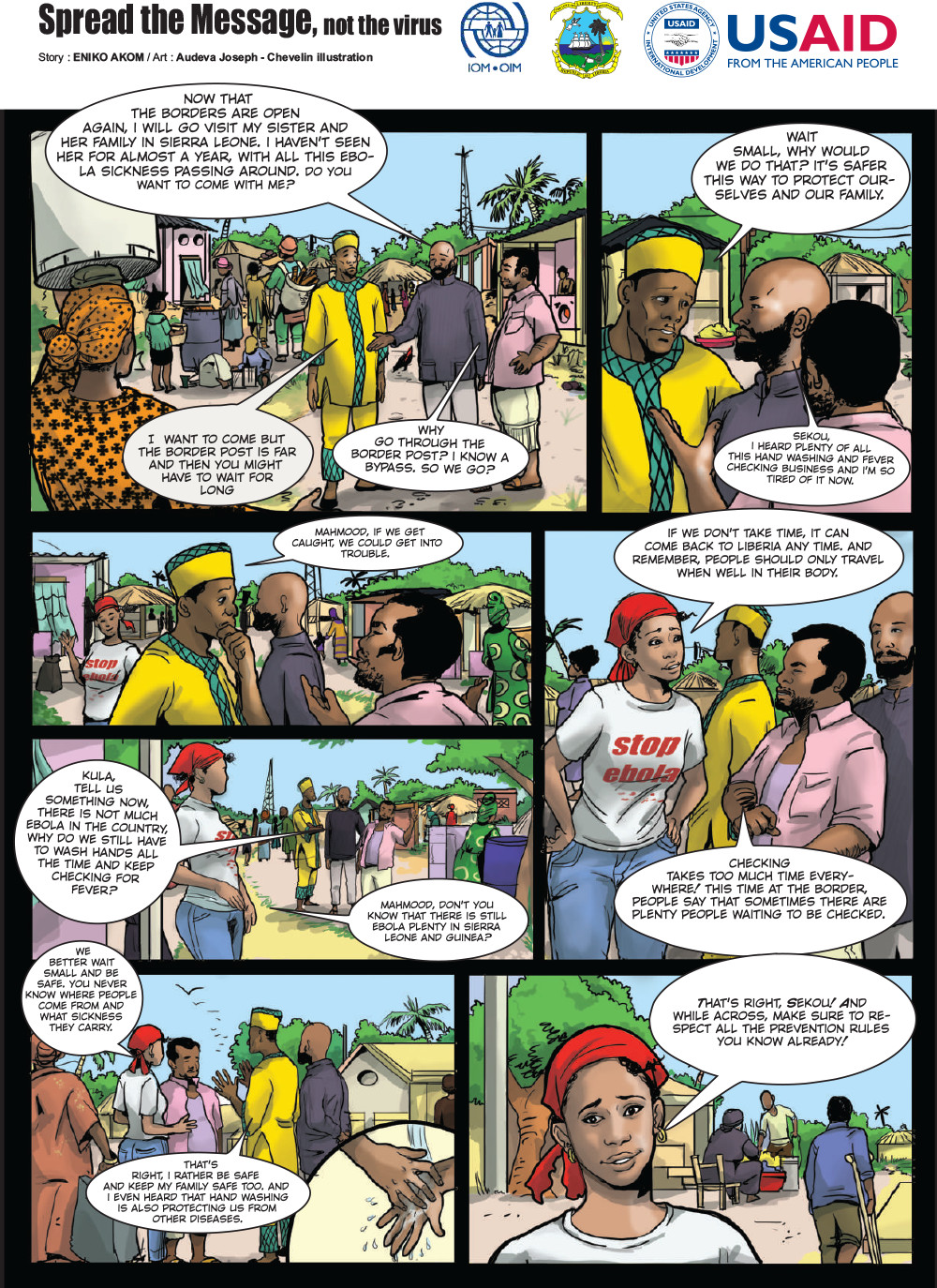
In September 2014, Ebola hit its peak in terms of death toll in Liberia, although that would not be apparent until later. Before significant international assistance arrived, SBCC materials and community and social mobilization were some of the only tools available to fight the virus and reduce cases. Village chiefs, and community and religious leaders became engaged and talked to their communities about the disease, stigma, prevention and treatment. Materials corrected misinformation and rumors and provided credible information. While Monrovia struggled, Lofa County was seeing a true decline due to its social mobilization efforts.

Click on an item to enlarge it

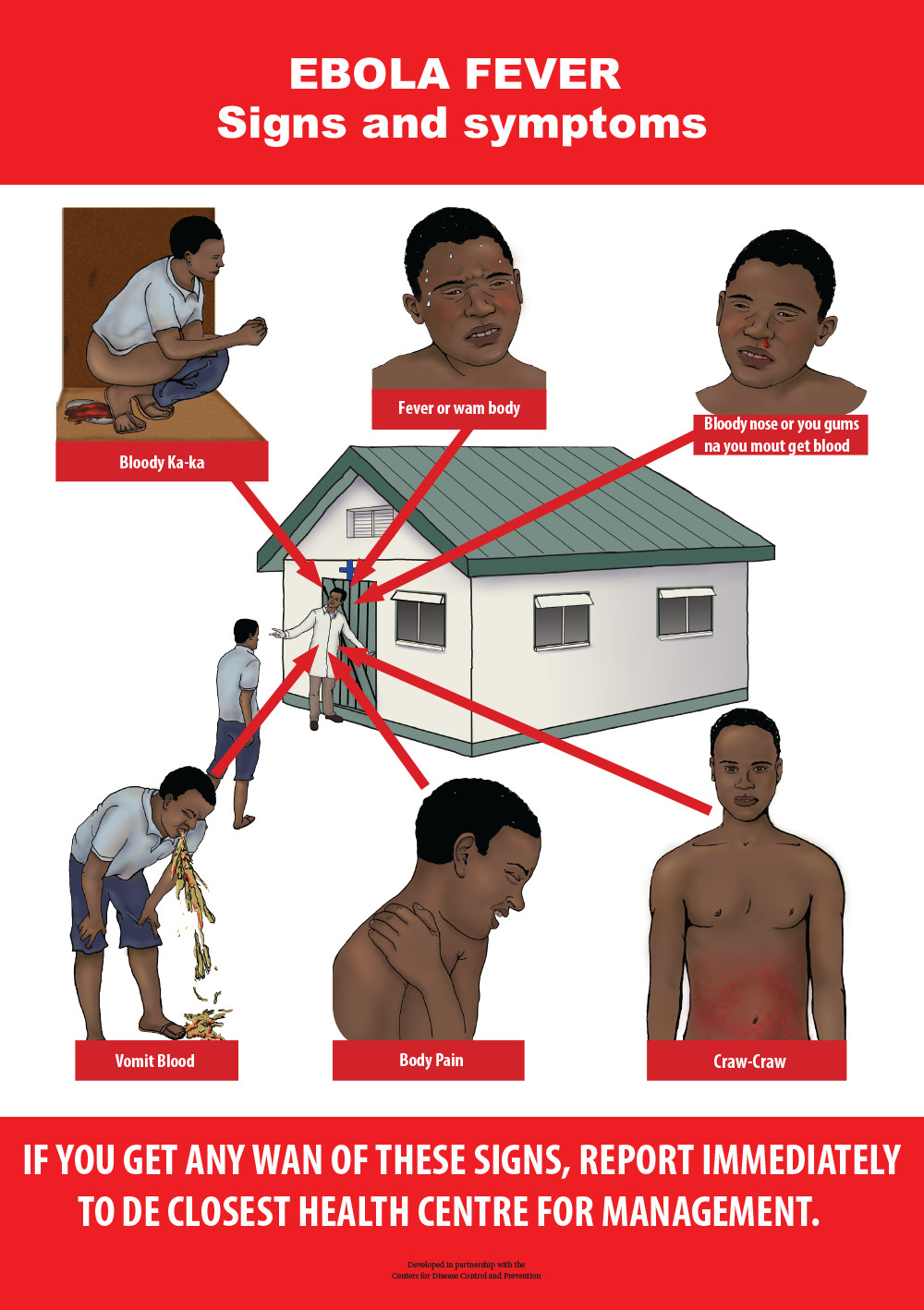

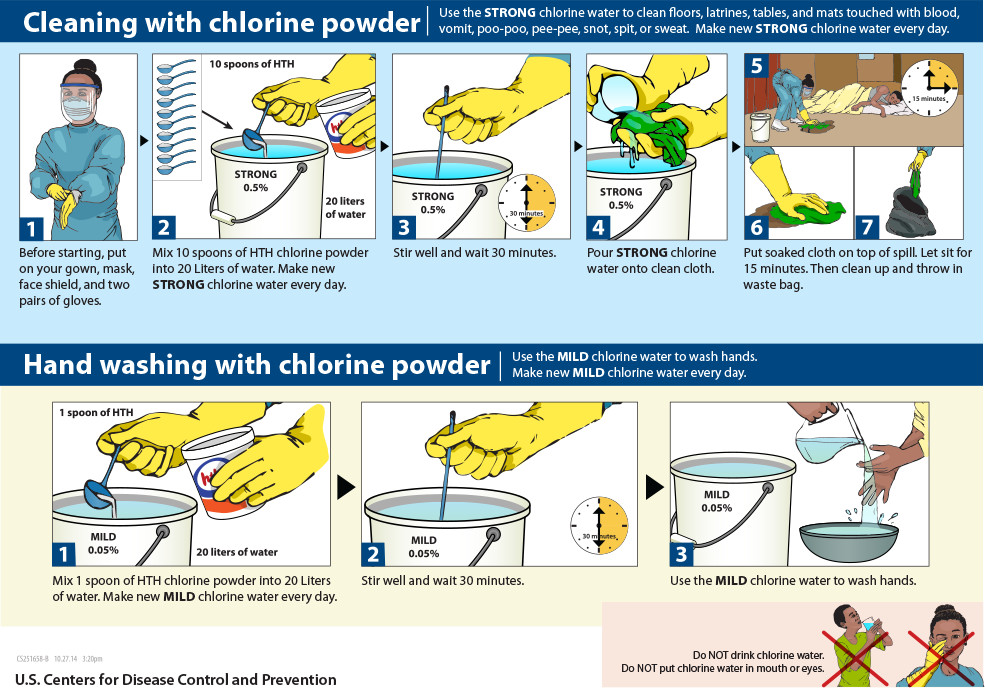

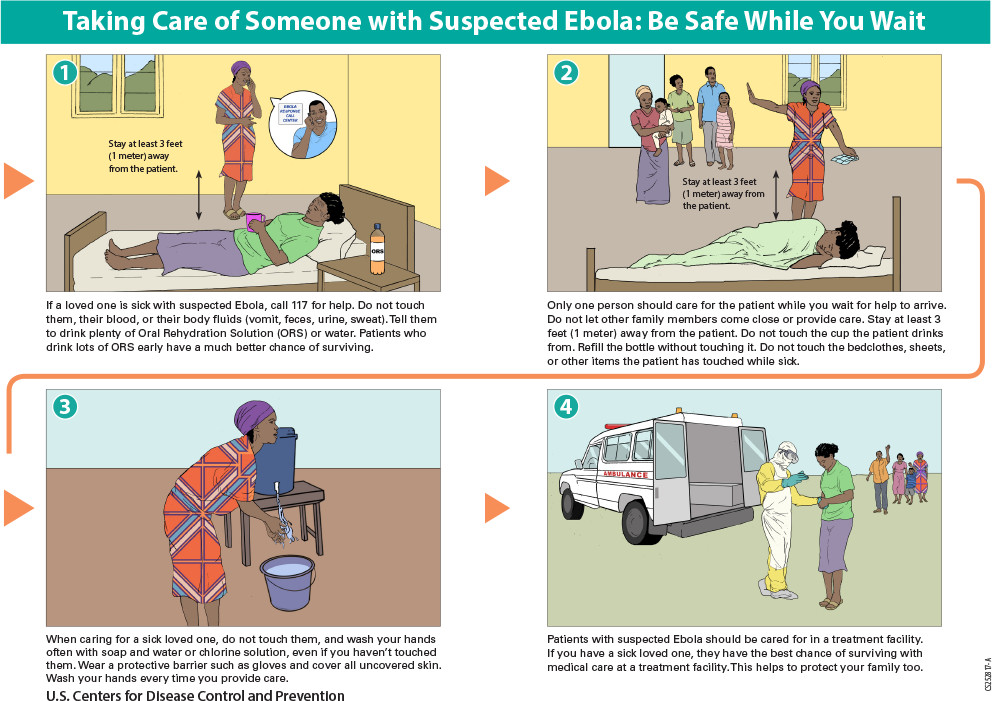
Radio was a critical channel for SBCC messages during the Ebola outbreak. HC3 produced six radio spots about Ebola in partnership with the Ministry of Health that aired in 18 local languages on 32 radio stations throughout the country. Among the messages were conducting safe burials, how to prevent the spread of Ebola, surviving Ebola through early treatment, what to do if you have signs and symptoms of Ebola, and what to do while waiting for help. The spots aired 120 times by each station during a period of 30 days and then again 240 times during a period of 60 days.
After Liberia was declared Ebola-free in May 2015, two additional radio spots addressing the need to remain vigilant aired in 18 local languages on 32 radio stations, with each station airing the spots 168 times during a 42-day period. The Ebola Community Action Platform also trained community radio stations to report their own stories and record their own Ebola spots.


In October 2014, the international community responded in force, and by November financial, material and human resources began pouring into the country. By this point, however, the number of cases and deaths began to subside (September and October were the peak months, by the end of November the number of cases per day had been more than halved). In December and January, newer Ebola treatment units (ETUs) were not filling to capacity. It was clear that behavior change through messaging and social mobilization was the primary driver of reduced infections and deaths, not the arrival of the new ETUs.

Source: WHO


On May 7, 2015, Liberia was declared Ebola free. But the celebration was short-lived. Six other cases emerged in June and July. The country restarted the countdown process and was again declared Ebola-free September 3, 2015. But after it flared up again in November, the country was declared virus-free in January 2016. Yet another case emerged in April 2016.


Reflecting on the trajectory of the outbreak underscores the need to incorporate SBCC in risk communication and emergency preparedness planning. While experimental vaccine trials for Ebola are now underway in West Africa and the health systems are undergoing an overhaul there, SBCC was all that was available at the start of the crisis in Spring 2014. SBCC can be applied to other emerging health threats such as Zika, as it has successfully been applied to existing threats like HIV/AIDS, malaria, child survival and maternal mortality.
Many of the same health organizations involved in the Ebola outbreak in West Africa are now working on SBCC programs and communication materials related to Zika. The Zika Communication Network is modeled after the Ebola Communication Network and houses materials for SBCC professionals to use as is or adapt for local needs. Below are some examples of materials now being used in Latin America to address behavior-related aspects of Zika.
Click on an item to enlarge it.