
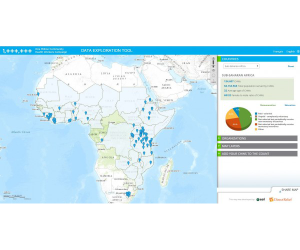
Direct Relief’s Data Visualization Tool for community health workers.
This case study is the first in a series of SBCC innovation case studies provided by HC3 partner NetHope.
Mapping Community Health Workers in Sub-Saharan Africa
Founded in 1948, Direct Relief is a nonprofit organization that provides medical assistance to people around the world who have been affected by poverty, natural disasters and civil unrest. Direct Relief works with healthcare professionals and organizations on the ground to equip them with essential medical supplies and equipment to help people recover from a disaster. Their research and analysis focuses on visualizing and communicating dense data and evaluating programs already in place. In particular, the department of research and analysis works with Geographic Information Systems (GIS) to present and communicate data.
Social and behavior change communication (SBCC) is a large part of Direct Relief’s work. The department utilizes GIS to collect data and then present data in a way that is digestible to its target population and other stakeholders. In addition, the maps are meant to highlight certain issues, particularly in health, that can provoke behavior change.
An interview with Dr. Andrew Schroeder, Director of Research and Analysis
Can you provide some background on the data tool project?
At the 68th session of the United Nations General Assembly, the successor to the Millennium Development Goals (MDGs) was discussed and established. The Sustainable Development Goals (SDGs) expands on the MDGs to integrate sustainable development into achieving international development goals, such as poverty alleviation, healthcare for all, combating climate change, and much more.
Community Health Workers (CHWs) have a large role in the SDGs. As an extension of the health system, CHWs have the power to bring more equitable distribution of health and medical supplies to countless individuals. In addition, by improving the health of women, it can directly lead to poverty alleviation, and improved educational outcomes. CHWs can also be a crucial force for changing behaviors to improve health. Since CHWs often closely interact with patients, the information they provide and recommendations they suggest can significantly alter health behaviors.
Hundreds of organizations work with CHWs in various parts of the world. These organizations may be a part of the government, private sector, or public sector. In order to develop standards for CHWs to adhere to, it is vital that we know where CHWs are located, what type of work they are doing, and which organizations they are doing it for. In collaboration with the One Million Community Health Workers Campaign, The United Nations and the Earth Institute at Columbia University have been working with Direct Relief to develop 10-12 mapping applications that can identify CHWs and provide necessary information for development agencies to understand the landscape of health in Sub-Saharan Africa.
What are the project’s objectives?
The objectives of this project are to:
- Identify and map CHWs in Sub-Saharan Africa
- Provide a snapshot of background information on CHWs including their affiliation, the services they provide, and the equipment they use or need
- Communicate this information quickly, efficiently and with effect to government or multi-lateral organizations to impact policy and funding
- Enable comparative analysis to understand which areas need more attention and resources than others in addition to identifying the strengths and weaknesses of the programs on the ground
Do you have any results to share?
The mapping application was shown at the United Nations General Assembly meeting in September and has been published here. The map has been accessed by hundreds of organizations across Sub-Saharan Africa that have identified and added CHWs in various countries.
How can we apply this to SBCC programs?
The use of GIS for mapping and data visualization has the power to communicate with various audiences in an effective manner. First, the project disseminated a survey to CHWs to integrate their responses onto the map. Then, the map and its resulting analysis serves as a mechanism to communicate with supplier networks to inform them of where medical supplies are need; to healthcare providers to understand where more CHWs are needed and their own strengths and weaknesses; to the general public to promote awareness of the issue; to donors to show them the cause and how to contribute; and, to experts in the field in order to strengthen overall health systems.
Particularly, there are several ways in which SBCC can be improved using GIS. If the public and donor organizations can clearly see where CHWs are working in the region, then they can create SBCC campaigns directed toward those workers to improve regional health outcomes. In addition, if there is an outbreak of a certain disease, then mapping the areas in which the disease is most prevalent can help prevent it from spreading. It can also be used as a persuasive tool to show the target population the real scope of the problem. By showing that HIV is very prevalent in a certain district can help promote preventative measures to be taken by those living in those areas.
The mapping application used in the project is interactive and is also able to receive communication from various stakeholders and audiences. Such interaction provides transparency and can ultimately be communicated to government officials and policy-makers to impact the way health is practiced in these areas. Communication to donor organizations is also of utmost importance in order to bring much-needed funding to Sub-Saharan Africa.
What are some of the lessons learned?
Direct Relief has been involved with several projects that incorporate GIS and mapping. One of the biggest lessons learned through their many years of expertise is that design matters. Although accurate data is vital, the manner in which data is presented is very important as well. Simply presenting numbers and statistics with no aesthetics or visualization techniques can cause people to tune out the issue entirely. Many public health issues that we deal with are obscure and abstract: data visualization can break these issues down so that a number of different audiences can relate to these concepts and can engage with the data itself.
There is also a tendency for developers of applications such as these to pack a lot of functionality into one application. The thought process might be that if you provide many different functions, the user will pick and choose what suits him or her the best. In fact, a lesson learned was to carefully think about how you want people to use the data and then design applications to do very specific things. In this way, people know right away what they are supposed to be doing with the application instead of having any confusion or moving onto something else entirely.
Finally, data visualization requires a design language. This language must be developed to speak to different groups of people. Direct Relief does not get the opportunity to test out their language, so it is careful research and understanding that is the backbone of how they design. By being observant of what different groups of people need, a mapping application can speak to a variety of audiences.
Dr. Andrew Schroeder is responsible for all analytics programs, monitoring and evaluation, data collection, business intelligence and data visualization, geographic information systems, and geospatial analytics. Schroeder has developed and implemented a number of projects at Direct Relief to demonstrate programmatic impact, including Mapping Global Prevention of Mother-to-Child Transmission (PMTCT) of HIV/AIDS; Spatial Analysis of the Global Diflucan® Distribution Program; development of GIS-based laboratory monitoring in Ethiopia; and USA Safety Net Mapping, which was cited in the New England Journal of Medicine. Schroeder has also presented findings from his research at Direct Relief at prominent conferences, including the Global Health Council and the InterAction Forum. Schroeder earned his Ph.D. in Social and Cultural Analysis from New York University and his Masters of Public Policy (MPP) from the Gerald R. Ford School of Public Policy at the University of Michigan, specializing in quantitative and qualitative social analytic methods, information technology policy and international development. Prior to Direct Relief he worked as an assistant professor of communications at the University of Wisconsin Oshkosh and as a research fellow in globalization and communications at the City University of Hong Kong.