
Behavior, such as going for an HIV test, is influenced by multiple factors or social determinants, often simultaneously. These include knowledge and attitudes about testing, perceived risk of HIV infection, self-efficacy to protect oneself from HIV, emotional reactions such as fear of transmitting HIV to an unborn child, and perceived social and gender norms around testing, among others. Understanding these behavioral drivers helps us influence them and better appreciate the complexities underpinning human decision-making. Strategically designed communication around HIV and AIDS, often referred to as social and behavior change communication (SBCC) or health communication, can influence all these factors in a positive direction.
Health communication goes beyond the delivery of a simple message or slogan to encompass a social process. People typically have more information than they can process and often do not make decisions taking all costs and benefits into account. Even after people accept information, they do not always act on it. Reducing barriers to action and making the long-term benefits of a behavior, adherence to ART for example, salient in the short term can enable people to take action and seek much-needed HIV-related services.
Among the powerful tools employed by health communication programs are community-level activities, interpersonal communication, quality counseling, information and communication technologies, new media and mass media. Health communication interventions are more likely to succeed when they use multiple coordinated communication elements to reach people with consistent high-quality messages through a variety of channels. When trying to understand the process of behavior change or develop an intervention, it is important to consider all levels of influence and related factors/determinants from the individual to structural while also relying on existing theories and comprehensive models to guide our work.
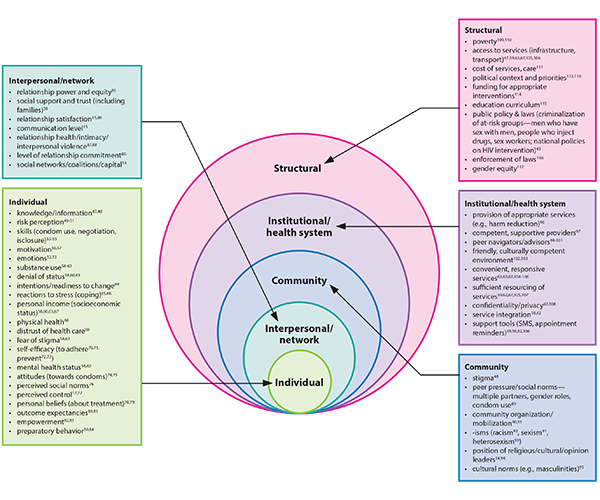
Figure 1: Kaufman, M. R., Cornish, F., Zimmerman, R. S., & Johnson, B. T. (2014). Health behavior change models for HIV prevention and AIDS care: practical recommendations for a multi-level approach. JAIDS Journal of Acquired Immune Deficiency Syndromes, 66, S250-S258.
Figure 1 outlines the various influences on behavior change at each level of the socio-ecological framework based on behavior change interventions related to HIV prevention, treatment and care.
Communication can be used to create health-seeking behavior, on the demand side, and as a means to improve the quality of in-service counseling, on the supply side. In the context of HIV, communication can motivate people to use condoms, seek voluntary medical male circumcision, get tested, obtain their results, promote access to treatment, link people living with HIV to care, support retention in care and help reduce stigma. The evidence in general points to health communication interventions as being cost-effective in achieving behavior change in many contexts, at least relative to the alternatives.
Research consistently shows evidence-based communication programs can increase knowledge, shift attitudes and cultural/gender norms, and produce changes in a wide variety of HIV-related behaviors.
With that said, communication interventions alone cannot overcome the challenges of HIV and AIDS in the absence of high-quality prevention and care services. But by the same token, biomedical interventions alone are unlikely to succeed without communication support that improves quality services and counseling, publicizes and explains these services and improves provider–client interactions, among other things. There are many complementary roles that health communication and biomedical prevention and care programs can play with numerous opportunities for synergy.
The database is a compendium of evidence to date that demonstrates the impact of health communication on HIV-related outcomes including:
- HIV Testing and Counseling (HTC)
- Voluntary Medical Male Circumcision (VMMC)
- Prevention of Mother to Child Transmission (PMTCT)
- Treatment Continuum
- Condom Use
- Other Prevention
Using data to ensure scientifically sound investments will yield the greatest impact, the evidence outlined here makes the case for the value of health communication across each core HIV intervention area as defined by PEPFAR 3.0. To reach the ambitious targets defined by PEPFAR and other global bodies, strategically deployed health communication is essential to improve HIV-related outcomes as demonstrated through the evidence in this resource. We hope this evidence is useful in your planning and implementation of high-impact interventions and approaches and welcome additional evidence for inclusion.
Process of Selection of Evidence for Inclusion
Evidence included in the database came from a rapid review of articles compiled for fact sheets previously published.
- Health Communication Impact on Condom Use
- HIV Testing and Counseling
- Impact of Health Communication Across the HIV Treatment Cascade
- The Impact of Community-Level Factors on Condom Use ).
Articles were included here if the study’s results showed the effects of one or more communication interventions on an HIV-related outcome. Searches were conducting using SCOPUS, PubMEd, PsychINFO, EBSCOhost and Popline. In addition to including relevant literature reviews, each article referenced within them was read to assess for individual inclusion as well. Researchers in several organizations were also asked to contribute program reports or other grey literature that showed the effects of communication on HIV outcomes. Four of these reports were included in the database. The criteria for inclusion and exclusion are listed below.
Inclusion criteria:
• Study was conducted in a low or middle income country (LMIC)
• Described a communication intervention or program; or was a synthesis or meta-analyses of HIV communication programs
• Reported on behavior change outcomes or intention for behavior change related to HIV outcomes
Exclusion:
• Were not in English
• Were not from a LMIC
• Did not report on a behavior change in at least one core HIV outcome area
• Did not focus on health communication aspects of an intervention