

Documenting SBCC’s Important Role in Malaria Case Management: Part II
 In August 2014, the Health Communication Capacity Collaborative (HC3) posted the blog, Documenting SBCC’s Important Role in Malaria Case Management, which described a gap in the documentation of impact evaluations for social and behavior change communication (SBCC) activities to improve malaria case management. Two potential contributing factors were discussed: failure to use standard SBCC malaria indicators in project design and evaluation, and a lack of focus on service providers as the target of SBCC interventions.
In August 2014, the Health Communication Capacity Collaborative (HC3) posted the blog, Documenting SBCC’s Important Role in Malaria Case Management, which described a gap in the documentation of impact evaluations for social and behavior change communication (SBCC) activities to improve malaria case management. Two potential contributing factors were discussed: failure to use standard SBCC malaria indicators in project design and evaluation, and a lack of focus on service providers as the target of SBCC interventions.
HC3 completed the desk review undertaken to better understand these two issues in May 2015. The Desk Review and Qualitative Assessment of Case Management Social and Behavior Change Communication Strategies in Four Countries: Ethiopia, Rwanda, Senegal and Zambia included a qualitative analysis (through key informant interviews (KIIs) in all four countries) of experiences and perceptions from the field, as well as a review of research, country-level documents, international publications and project reports.
Qualitative Analysis Details
Participants for KIIs were selected in the four countries and included members of the National Malaria Control Program (NMCP), SBCC/BCC units within the Ministry of Health (MOH), USAID implementing partners and President’s Malaria Initiative (PMI) staff.
KIIs took place from September to November 2014. When possible, interviews were conducted in person or via Skype; if not, written responses were obtained from the following information originally emailed to informants in order to prepare for their interviews. It was used to gather related perceptions and first-hand experiences with:
- Examples of activities promoting malaria case management messages.
- Effects of existing integrated case management of malaria programs and related SBCC approaches.
- Knowledge of the development process and input into any existing malaria communication strategy.
- Messages that have been particularly effective in changing knowledge, attitudes and practices related to malaria case management.
- The process for development of malaria case management materials.
- SBCC activities specifically at the community and/or facility level and audiences.
- What has worked best in SBCC for malaria case management.
- What SBCC foci should be considered in future malaria case management program design.
A log of the KIIs per country was kept and updated regularly within the team. In total, nine interviews, recorded and transcribed, and four written responses were collected, all of which were entered into NVivo 10. An initial codebook was developed based on the interview guide. Open and axial coding enhanced the initial codebook as themes were generated in the software.
SBCC for malaria case management in communities involves encouraging prompt care seeking behavior for those with fever, convincing people that it is important to test for malaria before medicating, and that if medicating for simple malaria with the recommended artemisinin-combination therapy (ACT), to take the full regimen as instructed. Among service providers, behaviors like clinical diagnosis (diagnosing based on symptoms, not based on blood results of rapid diagnostic tests or microscopy) and presumptive treatment with ACTs for those with fever must be addressed. This desk review describes a number of patterns in SBCC activities carried out to address community behaviors in Ethiopia, Senegal, Rwanda and Zambia.
One clear pattern documented in the review is that SBCC programming for malaria case management is not done as a stand-alone program or campaign. Unlike long lasting insecticide-treated net (LLIN) distributions and the SBCC campaigns conducted to support them, malaria case management behaviors are addressed as a part of broader malaria behavior programs and strategies. As such, it is rare to find a project or campaign evaluation that specifically examines the role SBCC played in changing malaria case management behaviors.
Another pattern found in each of the four countries were promising SBCC programs involving the Care Group model.
What are Care Groups
A Care Group is a group of 10-15 volunteer, community-based health educators who regularly meet together with project staff for training and supervision. They are different from typical mother’s groups in that each volunteer is responsible for regularly visiting 10-15 of her neighbors, sharing what she has learned and facilitating behavior change at the household level. Care Groups create a multiplying effect to equitably reach every beneficiary household with interpersonal behavior change communication. They also provide the structure for a community health information system that reports on new pregnancies, births and deaths detected during home visits.
This structure, used to change behavior at the community level, through community members themselves, has been used in a number of countries with different health programs. In this review the Kahebo Mwana program in Rwanda, the PECADOM Plus program in Senegal, the Chikankata Child Survival project in Zambia, and the Health Extension Package program in Ethiopia, utilized the Care Group model. The chart below (included in the review) provides details about the SBCC impact of each:
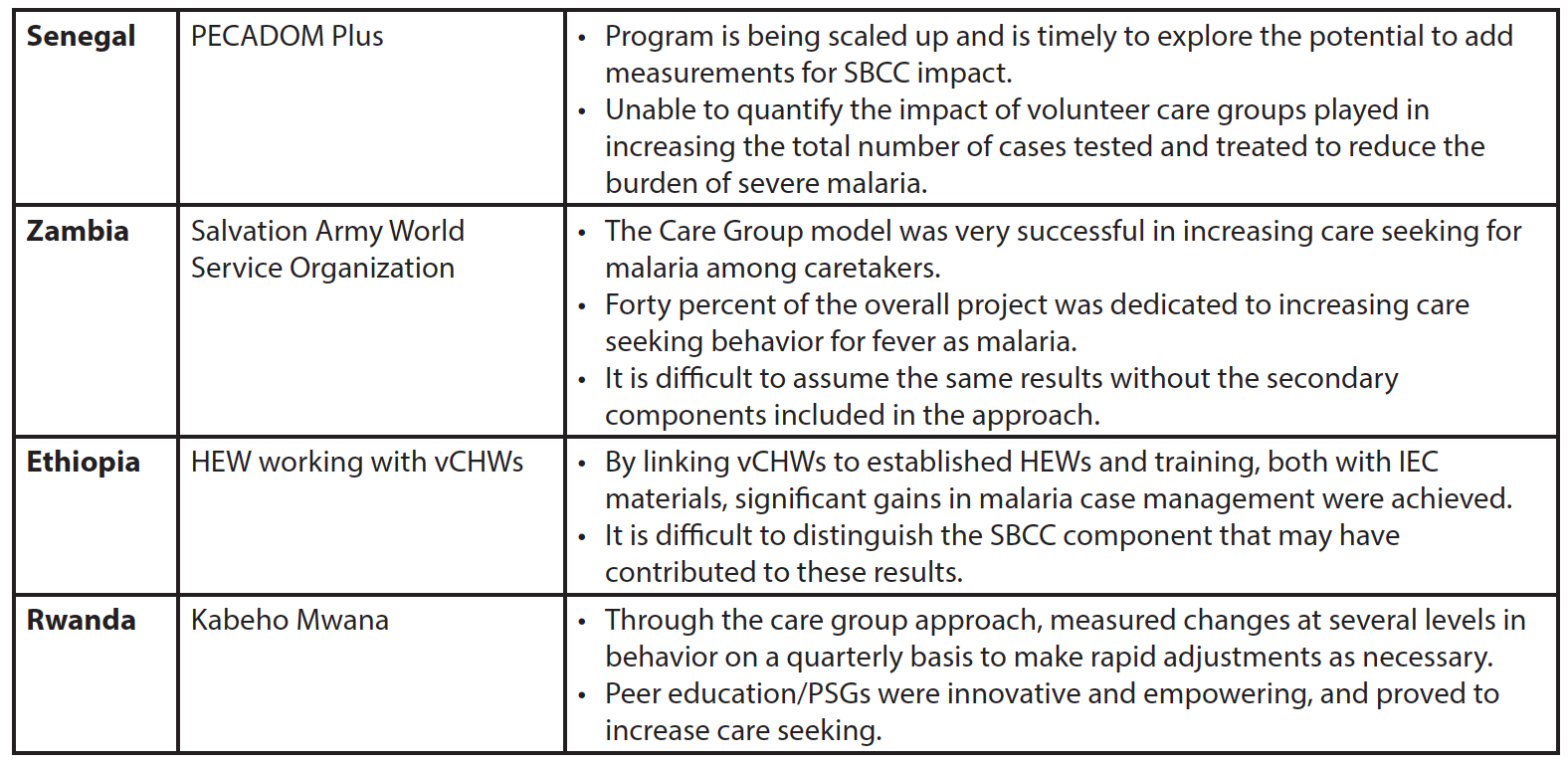
While Care Groups were identified as common components of promising programs, none of these programs evaluated the success of SBCC in particular, or attempted to measure the specific effect Care Groups played in changing behavioral indicators. Programs like Rwanda’s Kahebo Mwana program were successfully piloted and brought to scale, but much can still be learned about which environments and cultural contexts this approach may lend itself to.
Additional review recommendations include:
Include SBCC at inception: This review indicates most programmatic efforts to document SBCC activities’ contribution to malaria case management activities (in the countries reviewed) weren’t necessarily included at program inception, if at all. Malaria program coordinators and implementing partners should consider including SBCC personnel early in the program design phase, ensuring intentional, deliberate planning, monitoring and measurement of changes in knowledge and attitudinal behavioral determinants (for guidance, see the RBM Malaria BCC Indicators Guide).
Use inquiry to inform design: Formative research is a necessary component of any SBCC program or activity. Behaviors are highly localized in nature and change over time based on context. Findings from one country or region may not reflect behaviors in another. This is particularly true in malaria case management, where behaviors, such as treatment seeking, are influenced by seasons, malaria endemicity, and structural factors like availability of commodities and services.
Test Promising Practices: This review found a number of promising programs that used varying forms of care groups to organize CHWs and mobilize community members. While no deliberate effort has yet been made to determine what value SBCC contributed to these programs’ success, a systematic effort to introduce SBCC and measure its impact would be the first step in determining whether or not to use it. As the Rwanda Kabeho Mwana example shows, care groups have been successfully piloted and brought to scale (see care group selection criteria).
Evaluate the impact of SBCC: Pilots, programs and research reviewed found few examples of attempts to measure anything beyond SBCC inputs or outputs. This review has listed a number of SBCC programs implemented at different levels (community, regional, national) and paired them with appropriate methods of evaluation. While malaria case management programming is often one of many components in larger campaigns, it is possible to measure change in attitudes and behavior as a result of exposure to messaging.





Leave a Reply
Want to join the discussion?Feel free to contribute!