
Zimbabwe Fosters a Sense of Vigilance around Newly Acquired Malaria-Prevention Behaviors



 In 2000, Zimbabwe had a malaria incidence of 136 per thousand inhabitants. By distributing long-lasting insecticide treated nets (LLINs), spraying households with insecticide, encouraging prompt care seeking for fever and procuring accurate tests and effective treatment, the nation’s Ministry of Health and Child Care had succeeded in reducing this incidence rate to 29 inhabitants per thousand by 2015.
In 2000, Zimbabwe had a malaria incidence of 136 per thousand inhabitants. By distributing long-lasting insecticide treated nets (LLINs), spraying households with insecticide, encouraging prompt care seeking for fever and procuring accurate tests and effective treatment, the nation’s Ministry of Health and Child Care had succeeded in reducing this incidence rate to 29 inhabitants per thousand by 2015.
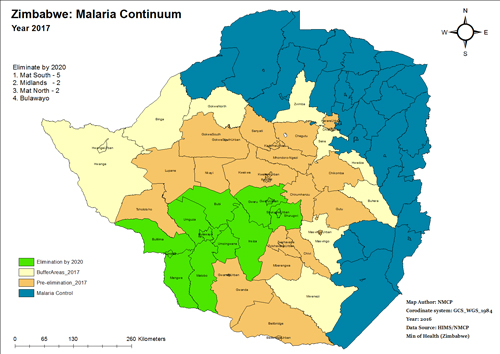
The National Malaria Control Program is working to expand the number of districts considered to be in the malaria pre-elimination phase (less than five cases per thousand inhabitants annually). One challenge the country faces is how to foster and maintain healthy malaria prevention behaviors while communities see fewer and fewer cases.
As communities watch school absenteeism rates fall, health care facilities see fewer cases of malaria in pregnancy and employers witness declines in sick days in the workforce, there is a danger that fear of malaria – an important motivator driving healthy behaviors – will fall as well. Without a means of communicating a sense of urgency among communities throughout Zimbabwe, there is a real possibility the healthy behaviors public health officials have worked so hard to establish will be reversed.
As exposure to malaria decreases, so does naturally acquired immunity.
In areas of pre-elimination, cases will be more severe, as immune systems once well-equipped to fight malaria struggle to fight it. Having fought so hard to encourage families to adopt appropriate preventive behaviors, Zimbabwe is now faced with the challenge of maintaining a sense of risk where it may be felt less and less with each passing year. New strategies and communication interventions are required to keep up with evolving perceptions about the risk of malaria and acceptance of new and unfamiliar testing and treatment methods. Communicating the need and rationale for the roll out of different interventions between neighboring communities will be necessary. Cross-border efforts will need to address different levels of malaria transmission and complimentary policies between different countries.
Finally, an effort to reach special populations such as travelers, traders, itinerant laborers and difficult-to-reach minority groups will become increasingly important. This past January, the Health Communication Capacity Collaborative (HC3) guided government officials and their partners from around the country through how best to encourage families and communities in control and pre-elimination districts alike to achieve a malaria-free country.
 In a participatory process that lasted five days, central and district level health promotion officers, national malaria control program personnel, national and international partners took part in a workshop that focused on prioritizing behaviors and then using available data and experience to determine root causes of these behaviors and the most likely means with which to influence each. Led through the five-step P-Process by HC3 program officers Mike Toso and Angela Acosta, stakeholders developed situation analyses to describe where they are, participated in a shared vision exercise to determine their goals for the future and reviewed data from several household surveys, program reports and peer-reviewed articles to determine specific behavior and communication objectives to be tailored to target audiences.
In a participatory process that lasted five days, central and district level health promotion officers, national malaria control program personnel, national and international partners took part in a workshop that focused on prioritizing behaviors and then using available data and experience to determine root causes of these behaviors and the most likely means with which to influence each. Led through the five-step P-Process by HC3 program officers Mike Toso and Angela Acosta, stakeholders developed situation analyses to describe where they are, participated in a shared vision exercise to determine their goals for the future and reviewed data from several household surveys, program reports and peer-reviewed articles to determine specific behavior and communication objectives to be tailored to target audiences.
Once broad-view decisions about priority behaviors and national-level approaches to influence them were made, a smaller group of national malaria control program officers and several partners spent an additional five days reviewing data, developing communication plans to influence prioritized behaviors and framing country progress and aspirations for the future. The team reviewed a number of social and behavior change communication (SBCC) theories, models and results frameworks to better describe the link between this strategy’s approaches and expected impact on health outcomes.
The result of this work is Zimbabwe’s new Malaria Communication Strategy 2016-2020. Several highlights of the new strategy include:
- Malaria communication plans for SBCC activities supporting surveillance, cross-border activities and special populations
- Specific focus on behavior and communication objectives for traditional and religious healers
- Specific SBCC approaches and implementation considerations for high to moderate, and low malaria transmission areas
- An implementation guide that includes partner activity mapping and an implementation timeline
- Guidelines and next steps for the creation of a malaria branding strategy
- A monitoring and evaluation plan developed to track and evaluate progress on the highest priority behaviors over then next four years
The draft strategy is in the process of being validated. Once feedback has been received and the National Malaria Control Program has made final decisions regarding final inputs, the document will be sent to the Ministry of Health to be signed. Look for the finalized document, as well as other strategies collected, in HC3’s malaria communication strategy map.

Break-out sessions enabled small groups to focus on behavior specific communication plans.

One exercise completed in small groups was a “root cause analysis.”
The Zimbabwe National Malaria Control Program and partners gathered in Harare.






{kind=link}
Leave a Reply
Want to join the discussion?Feel free to contribute!