
Recap of Improving HIV Outcomes through Health Communication Webinar
HC3’s March 26 webinar on Improving HIV Outcomes through Health Communication was based on articles to be published in a supplemental issue of JAIDS planned for a July release. The webinar is the first in a series of four focused on HIV and health communication.
Douglas Storey, PhD, Director for Communication Science and Research at the Johns Hopkins Bloomberg School of Public Health Center for Communication Programs (JHU∙CCP) gave an overview of health communication, noting that it is a subset of communication science that grew out of disciplines, such as psychology, sociology as well as neuroscience. Communication is a process, he said, which has four major functions:
- To inform about something
- To persuade or encourage
- To connect with other people
- To express and maintain culture (communicate about shared values)
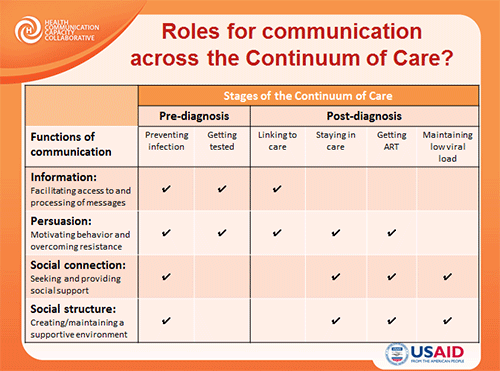 Dr. Storey also discussed how communication plays a role at each stage of the HIV continuum of care. For example, providing information and informing people is one of the most important activities in the first stages of the continuum, while social structure comes more into play when behavior needs to be reinforced.
Dr. Storey also discussed how communication plays a role at each stage of the HIV continuum of care. For example, providing information and informing people is one of the most important activities in the first stages of the continuum, while social structure comes more into play when behavior needs to be reinforced.
Dr. Blair Johnson, Professor of Psychology at the University of Connecticut, presented evidence from meta-analyses examining behavioral interventions conducted around HIV risk reduction. His team at the University of Connecticut has found 56 meta-analyses around behavioral interventions for HIV prevention to date, demonstrating the wealth of data available on this topic. Efficacy has been found to vary from study to study and a lot of heterogeneity has been found. Interventions that tend to succeed were found to use strategies that target specific populations and also take into account community-level factors that may impact behaviors.
Dr. Johnson then introduced the concept of behavior change technique taxonomies (BCTs) that has developed over the last 10 years. BCTs offer greater precision in identifying behavior change components and provide a way to consistently label across studies. To date, no meta-analysis has used BCTs but as they become used more often, they should be able to provide better insight into the reasons for discrepancies across trial results, easier replication of trial results and a way to more readily translate finding into communities.
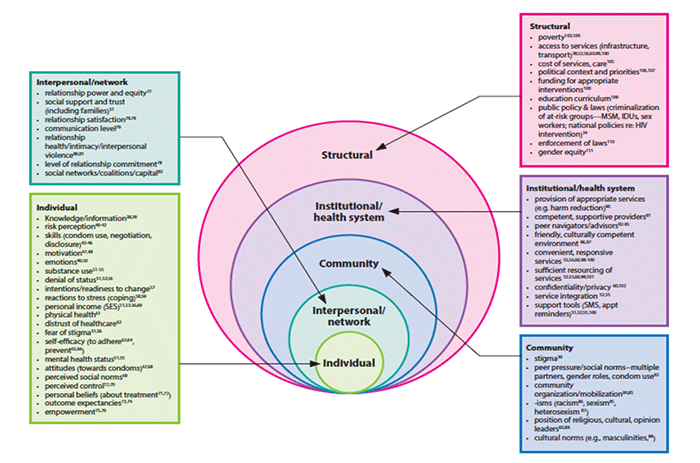
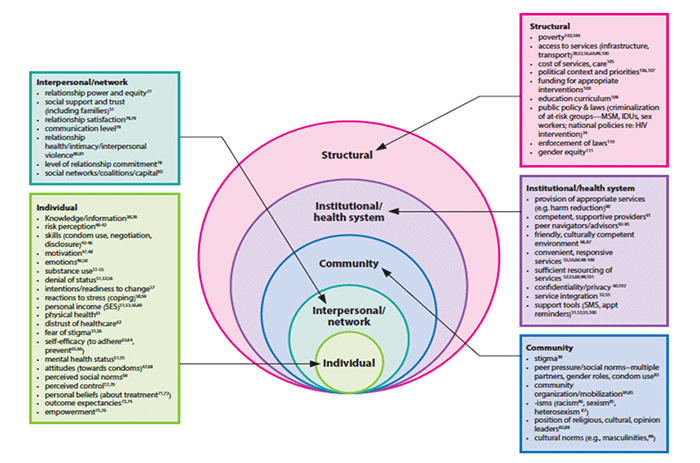 Dr. Michelle Kaufman, JHU∙CCP Research and Evaluation Officer focused on the big picture with her presentation, noting a shift towards including social and structural determinants of HIV-related behavior in individually focused intervention programs to get closer to the goal of no new infections. Dr. Kaufman and her colleagues have created a menu of HIV behavior change factors and placed them across the socio-ecological model to show different factors to consider at each level. It includes those factors at the individual, interpersonal, community, institutional and structural levels, with examples such as relationship power and equity at the interpersonal level, and education curriculum at the structural level. Dr. Kaufman also highlighted three newer models that take individual level theories shown to be successful in the past and expand some of their aspects to higher levels. These include:
Dr. Michelle Kaufman, JHU∙CCP Research and Evaluation Officer focused on the big picture with her presentation, noting a shift towards including social and structural determinants of HIV-related behavior in individually focused intervention programs to get closer to the goal of no new infections. Dr. Kaufman and her colleagues have created a menu of HIV behavior change factors and placed them across the socio-ecological model to show different factors to consider at each level. It includes those factors at the individual, interpersonal, community, institutional and structural levels, with examples such as relationship power and equity at the interpersonal level, and education curriculum at the structural level. Dr. Kaufman also highlighted three newer models that take individual level theories shown to be successful in the past and expand some of their aspects to higher levels. These include:
- Multiple Domain Model
- Network-Individual Resource Model
- Dynamic Social Systems Model
Dr. Kaufman concluded with the following five recommendations on how communication can take multiple levels of behavior change factors into account:
- Consider all levels of influence, from individual to structural, when trying to understand behavior change or develop an intervention.
- Consult with colleagues in different fields that may see things differently and be able to make recommendations.
- Measure, test or intervene at least 2 levels.
- Where possible, combine already existing theories at various levels.
- Be sure to consider the scalability and sustainability of an intervention.
To learn more, check out the JAIDS supplement to be published at the beginning of July, where each of these speakers will expand upon these ideas in their articles. You can also join our Health Communication Community by signing up to receive updates from the HC3.
If you would like to watch the entire webinar or view the presentations in PDF, click on the Webinar Resources box below.
[toggle title=”Webinar Resources” load=”hide”]
Presentations:
The Role of Communication Across the HIV/AIDS Continuum of Care, Doug Storey, PhD
Behavioral Interventions for HIV Prevention: Role of Message Content, Blair T. Johnson, PhD
Multi-Level Approaches to Changing Behavior for HIV Prevention and AIDS Care, Michelle R. Kaufman, PhD
Additional References:
Use of Mass Media Campaigns to Change Health Behaviour
The Behavior Change Technique Taxonomy (v1) of 93 Hierarchically Clustered Techniques: Building an International Consensus for the Reporting of Behavior Change Interventions
Standard Care Impact on Effects of Highly Active Antiretroviral Therapy Adherence InterventionsA Meta-analysis of Randomized Controlled Trials
Adherence & HIV: Presentation from Marijn de Bruin at CHIP describing his BCT work.
Addressing the Slow Uptake of HIV Testing in Malawi: The Role of Stigma, Self-efficacy, and Knowledge in the Malawi BRIDGE Project
Stigma Against People with HIV/AIDS in Rural Ethiopia, 2005 to 2011: Signs and Predictors of Improvement
HIV/AIDS Care Continuum
Progress Along the Continuum of HIV Care Among Blacks with Diagnosed HIV— United States, 2010 [/toggle]
Questions and answers from the Improving HIV Outcomes through Health Communication webinar have been posted here.
Dr. Doug Storey’s Presentation:
[accordions ]
[accordion title=”Q: What is the reason for not choosing social structure/connection and information in some of the cascade stages?” load=”show”]A: There probably are roles for each of the functions of communication at each stage of the continuum, but some may be somewhat more important at some stages than others. The point is to think strategically about how to use communication at each stage and not use it indiscriminately.[/accordion]
[accordion title=”Q: How can the different forms of communication be used to maximize impact at each stage of the continuum of care?” load=”hide”]A: There is growing evidence of communication impact at all stages of the continuum, some more than others. The key is formative research about the ideational factors that facilitate or constrain behavior at a specific stage and for a particular audience, then design communication activities to address those factors, either strengthening the positive ones or changing the negative ones.[/accordion]
[accordion title=”Q: What do you see as the role of feedback (listening) as a function of understanding and speaking to relevant audience core values?” load=”hide”]A: Communication is a two-way process. Listening is a critical aspect of communication that creates and reinforces a relationship between the communicators and improves the effectiveness of the interaction.[/accordion]
[accordion title=”Q: How should we address issues related to disclosure of HIV status when communication is happening at the group/social network level?” load=”hide”]A: It depends on the goals and purpose of the intervention. In a group setting it is always important to set ground rules for the discussion. And sometimes, in a focus group discussion, for example, we would try not to mix HIV+ and HIV- individuals.[/accordion]
[/accordions]
From Dr. Blair Johnson’s Presentation:
[accordions ]
[accordion title=”Q: Given the heterogeneity of interventions in the meta-analysis, what are some of the major lessons learned from the more promising interventions and/or differences from those that were not as successful?” load=”show”]A: Behavioral skills (condom skills training) come up a lot in these meta-analyses and motivational training also seems to be successful. Because BCTs weren’t used though, there have been different definitions in the past by people making it hard to compare across studies. Dose response is rare to be shown in meta-analysis. In future we hope to see specific BCTs correlated as well as the intensity, we need to get be specific about the dose response because at some point it probably will level off but we need to find that point.[/accordion]
[accordion title=”Q: What has De Bruin used as communication strategy to succeed in maintaining patients under ART treatment?” load=”hide”]A: His work gauged how much social support ART patients were given, it was a broad set of BCTs. Here is a link to the de Bruin work: http://bit.ly/P0tFrn and here is a talk that de Bruin gave at CHIP that describes his BCTs quite clearly. http://www.chip.uconn.edu/chipweb/lectures/20091001_Marijn_De_Bruin/Presentation/MBruin.ppt[/accordion]
[accordion title=”Q: Considering the heterogeneity as presented in Dr. Johnson’s session, doesn’t that indicate the difficulty of ‘scaling up’?” load=”hide”]A: The short answer is yes. To reword the question, if interventions effectiveness is varying across trials then wouldn’t that mean translating the results more difficult? And yes that is true, that’s why we need meta-analyses to try and make sense of these different results to be able to translate it effectively. We can’t just race ahead because one trial was effective. There are many factors that play a role; we need to figure out what those are so that we can scale up effectively to communities.[/accordion]
[accordion title=”Q: To what extent are the findings from meta-analyses impacted by confirmation bias – where findings that fail to reject the null (no efficacy) are not published?” load=”hide”]A: Publication bias seems rare in HIV prevention research.[/accordion]
[/accordions]
From Dr. Michelle Kaufman’s Presentation:
[accordions ]
[accordion title=”Q: Where on the menu of behavior change factors would we find personal priorities; i.e., what matters most on an individual’s priority scale?” load=”show”]A: There isn’t anywhere where its specifically listed as personal priorities but motivation and some of the personality characteristics and relationship factors, personal commitment may fall into this category.[/accordion]
[/accordions]
General Questions:
[accordions ]
[accordion title=”Q: Why, since we know how much stigma against PLHIV affects treatment, do we not address stigma with BCC programs as we do for BCC prevention?” load=”show”]
A: There are some interventions that do look at this and try to bolster the pride of the people in the intervention since they are members of a stigmatized group. Some of the research done on the Malawi BRIDGE project looks at this. It was a radio diary project that gave HIV+ individuals an opportunity to talk from a personal perspective about how they were dealing with their HIV status, social relationships and their adherence to treatment. The intervention was designed to put a human face on those living with HIV and AIDS and there’s been research done that looks at the changes in public perception of people living with HIV based on that. You can find more information here http://www.jhuccp.org/sites/default/files/Berendes%20Testing%20JANAC.pdf
Here is an article on factors related to decreased stigma seen in Ethiopia: http://link.springer.com/article/10.1007/s10461-013-0611-0[/accordion]
[accordion title=”Q: What has the field of neuroscience contributed to the information presented in the three presentations?” load=”hide”]
A: It doesn’t have much influence on risk reduction strategies to date. Looking at AIDS patients and how they reply to different communication strategies could be done but we don’t see it as a practice in a field. In theoretical practice it could be possible but we are not aware of any work being done towards this.
[/accordion]
[/accordions]





Leave a Reply
Want to join the discussion?Feel free to contribute!