

Building a Virtual Document Repository with Health Educators in Sierra Leone
Over Skype, I listened to the HC3 team in Sierra Leone as they shared ideas for developing a virtual document repository. The need to organize virtual and paper-based documents had been identified by the Ministry of Health and Sanitation’s (MOHS) Health Education Division (HED). Health promotion materials and resources, they said, were too hard to find, difficult to access and not often in the form they wanted. As a knowledge management expert this was a problem groups from Nigeria to Tanzania had described to me many times before, but one that required a customized solution. Since I was in the U.S. and had a weak grasp of how work was conducted in a country I was going to for the first time, I listened to my teammates’ suggestions closely.
I knew that a decade of civil war, ending in 2002, contributed to a health system that struggled to address numerous issues including a maternal mortality rate among the highest in the world. I also knew that the Ebola epidemic that hit West Africa last year capitalized on this fragile health system and pushed it over the edge.
 Thankfully, after an all-out effort led by the Ministry and supported by key partners, WHO announced an end to the public health emergency in March of this year. After this declaration, the difficult task of rebuilding confidence in the health sector picked up steam. HC3 took a lead role in these efforts and quickly recognized that knowledge management had a role to play in driving the recovery and reconstruction phases.
Thankfully, after an all-out effort led by the Ministry and supported by key partners, WHO announced an end to the public health emergency in March of this year. After this declaration, the difficult task of rebuilding confidence in the health sector picked up steam. HC3 took a lead role in these efforts and quickly recognized that knowledge management had a role to play in driving the recovery and reconstruction phases.
Throughout the five phases of emergencies, knowledge management can be used to develop or improve systems for collecting, organizing and sharing tacit experiences and explicit resources. These systems can also be used to reinforce the foundations built to address the emergency and serve to broaden cooperation and collaboration and address related issues. In the event that a similar emergency occurs, a strengthened system can help ensure that related knowledge and resources are easily accessible and available.
These KM capacities and strengths were the same ones that resonated with the HED and HC3 teams as they juggled multiple activities with several partners on a daily basis. They realized a significant amount of knowhow was accumulating at the HED’s central office and there was limited opportunity to categorize and share it.
Hard copy vs. soft copy: a false dichotomy
HED staff in Sierra Leone conducted work in both physical and virtual spaces but neither were used systematically to disseminate knowledge. There was adequate internet connectivity and enough staff with phones to make virtual communication appealing, but many aspects of official work was still conducted in hard copy. The value of working in hard copy was also reflected in a sentiment shared with me by a district social mobilization coordinator: “If a partner wants our attention, bring us a hard copy.”

HED staff member Ben Coker presents a possible system for organizing files in the virtual document repository.
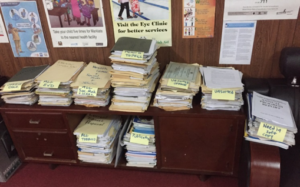
These dual communication efforts presented a knowledge management challenge that I began to address through a review of the hard copy files in the HED office. This amounted to about 10 years of memos, meeting notes, draft strategies and health promotion products. My informal canvas of the health topics being addressed at the HED office indicated that three topics were dominant: Ebola, tobacco control and vaccination campaigns. In addition, there were significant health promotion and SBCC materials that covered a wide spectrum of topics including alcohol abuse, HIV and cholera.
 Next, I looked at the results from an assessment that the HC3 team conducted on knowledge-sharing practices a few months before my visit. In particular I was interested in the virtual spaces already being used that could be built upon. What we realized was that most staff kept electronic files on their desktops and shared them only via email and flash drives. Neither were a great way to keep and share documents due to hardware reliance and space issues.
Next, I looked at the results from an assessment that the HC3 team conducted on knowledge-sharing practices a few months before my visit. In particular I was interested in the virtual spaces already being used that could be built upon. What we realized was that most staff kept electronic files on their desktops and shared them only via email and flash drives. Neither were a great way to keep and share documents due to hardware reliance and space issues.
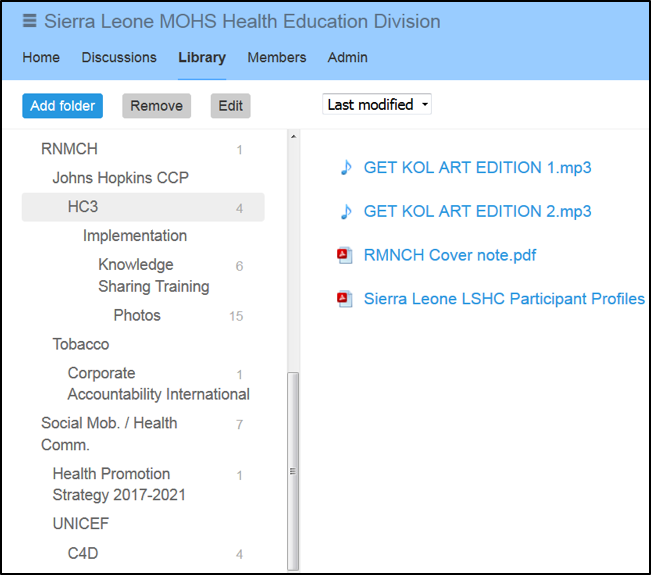
I decided to introduce a new platform like Dropbox and Google Drive to host the virtual document repository. But instead of these popular tools, I chose a platform built for the health and development sector. The Knowledge Gateway, built by WHO over 10 years ago, has been used by over 300,000 people. It has stood the test of time due its straightforward functionality and capacity to serve in low bandwidth settings. The platform is also free to use and thus is a great introduction to virtual centralized sharing tools for a group dependent mostly on email.
Developing a taxonomy
Four HED staff at the central level were joined by 13 district social mobilization coordinators at an HC3 workshop that outlined key benefits of knowledge management, the functionality and architecture of the Knowledge Gateway, and the steps to develop a virtual document repository.
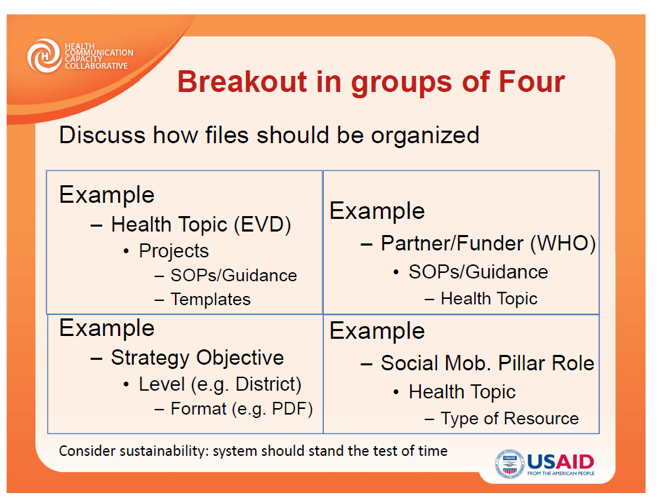
A key step that was discussed centered on the structure of file types, also known as taxonomy. To do this, the group broke into teams of four and developed a sample hierarchy that they then shared with the wider group.
After discussing the different ways of organizing their resources, the group settled on a system categorized first and foremost by health topic and, secondarily, on funding source. Once the structure was complete, the group engaged in an exercise to help populate the repository.
Populating the repository
The group again broke into small teams and were asked to make four lists based on the questions below:
- What are the top three documents you consult on a regular basis?
- What are the top three documents you think new staff should have access to?
- What are the top three documents that you want greater access to?
- What are the three topics/processes you want to see documented and shared?
 With these results, the group decided 15 resources should be initially uploaded and then identified who among them had soft copies. Among these resources were the HED Partner List, the 2013 DHS Report, the MOHS Basic Package for Health Services, and the Ebola Recovery Plan. They also identified the draft of the new 2017-2021 Health Promotion Policy that HC3 is helping to develop. In a few cases, soft copies were not available but hardcopies were available in the HED office.
With these results, the group decided 15 resources should be initially uploaded and then identified who among them had soft copies. Among these resources were the HED Partner List, the 2013 DHS Report, the MOHS Basic Package for Health Services, and the Ebola Recovery Plan. They also identified the draft of the new 2017-2021 Health Promotion Policy that HC3 is helping to develop. In a few cases, soft copies were not available but hardcopies were available in the HED office.
The day after the workshop, with the aid of a high-speed scanner, we converted some of these paper resources to digital versions and made them more accessible to a larger group of stakeholders by posting them in the HED Knowledge Gateway.
At the end of my trip, the relationship between hard and soft copies had been clarified and strengthened at HED. Their next knowledge management challenge is to establish guidelines that formalize how resources and materials should be collected and shared among other HED partners and stakeholders, no matter what form they take.






Leave a Reply
Want to join the discussion?Feel free to contribute!